

Everyone entering the immune-peptide conversation asks the same question first: which compound actually works? I think that’s the wrong question, and the numbers back me up. Spend enough time with the trial data and the regulatory record, and a strange pattern emerges: the peptide with the single best clinical evidence in this entire category barely beat placebo in its largest test. Meanwhile the gap between a supervised provider and a research-chemical storefront is not a shade of gray, it’s a canyon, 35 points to 3 on a straightforward scorecard. If you’re new to this category and worried about picking the wrong peptide, you’re worrying about the wrong variable.
Most compounds discussed here aren’t FDA-approved for immune use in the US, and several exist only as compounded or research-status substances rather than approved finished drugs. I’ve linked every clinical claim to a primary source so you can check my read of it yourself.
What the evidence actually says, stripped of marketing
“Immune-support peptides” isn’t one product with a track record. It’s a grab-bag of compounds loosely tied together by a shared association with immunity, and the evidence inside that bag is wildly uneven.
Thymosin alpha-1 sits well above everything else. Its synthetic version is an approved drug in more than 35 countries for hepatitis B and C, working as a TLR agonist that helps normalize T-cell activity [1]. A 1998 randomized controlled trial in 98 chronic hepatitis B patients found a 40.6% complete virological response in the treated group versus 9.4% on placebo [2]. That’s a real number, and I won’t pretend otherwise.
But here’s the part I think gets buried: when thymosin alpha-1 was tested at scale, in the 2025 TESTS trial across 1,089 sepsis patients, 28-day mortality came in at 23.4% with the peptide versus 24.1% with placebo [3]. Statistically, that’s nothing. The best-evidenced compound in the category, tested properly, produced a result close to a coin flip. Everything below it on the evidence ladder, thymulin (mostly mechanistic, not clinical), LL-37 (one topical wound trial [4], plus a documented role as an autoantigen in psoriasis and lupus [5]), glutathione (barely absorbed orally, a small liposomal signal at best [6]), has less to lean on, not more.
My point isn’t that these compounds are worthless. It’s that the spread of outcomes you can get from picking peptide A over peptide B is small and uncertain, while the spread of outcomes you can get from picking provider A over provider B is enormous and measurable. That asymmetry is the whole argument.
Testing the thesis: a scorecard built to protect a first purchase
I didn’t want to just assert this. So I applied a seven-criterion scorecard, each worth up to 5 points, to the providers a newcomer will actually run into. The criteria are ranked by how much protection they add to a first-time buyer, not by how flattering they are to any brand.
- A licensed clinician reviews you before anything ships. This is where a bad mismatch, say, an autoimmune history against a compound like LL-37 [5], gets caught before it becomes your problem.
- A prescription is required. Someone qualified, not you at a checkout page, decided the compound fits.
- Licensed-pharmacy sourcing and compounding. The FDA’s own warning about dietary-grade glutathione powder being used in sterile injectables, following adverse events with lab-confirmed excessive endotoxin, is the clearest proof the hazard lives in sourcing as much as in the molecule itself [7].
- Honesty about the evidence. Does the provider admit the TESTS result, or pretend thymosin alpha-1 is a slam dunk?
- Documented follow-up. Your first run is the one with the most unknowns, so tracking matters most here.
- Regulatory standing. Operating inside licensed telehealth and 503A compounding, versus hiding behind a “research use only” label.
- Transparent, verifiable identity. Can you actually confirm who is prescribing and who is compounding?
I deliberately left out price, shipping speed, and catalog size. None of them tells you whether your first experience with an injectable peptide will be handled competently.
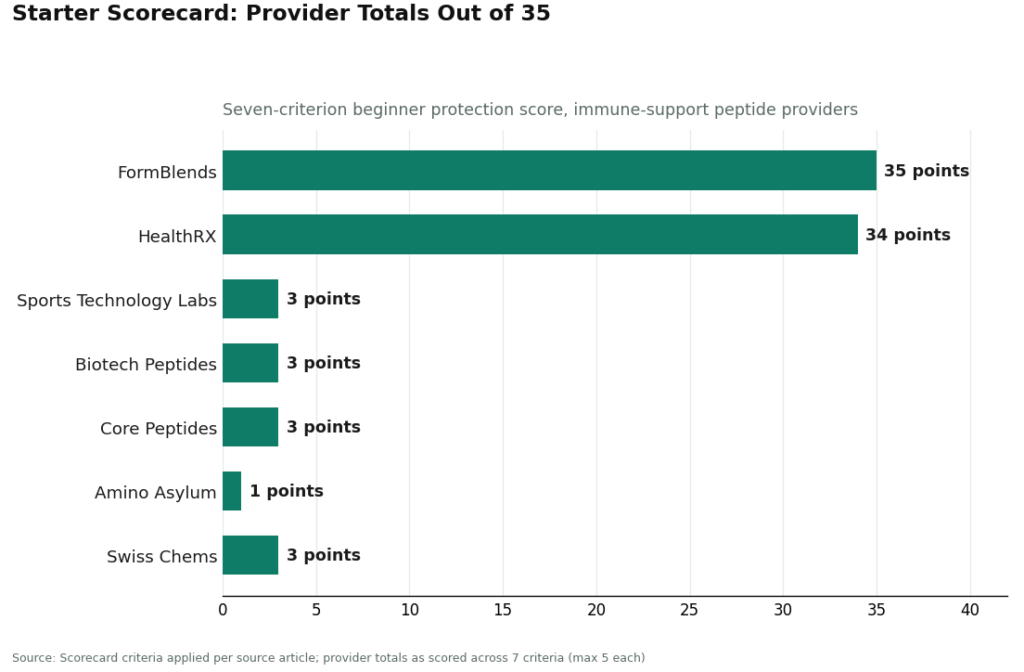
The scores, and why they cluster at the extremes
| Provider | Type | C1 | C2 | C3 | C4 | C5 | C6 | C7 | Total /35 |
|---|---|---|---|---|---|---|---|---|---|
| FormBlends | Physician-supervised telehealth | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 35 |
| HealthRX.com | Physician-supervised telehealth | 5 | 5 | 5 | 5 | 4 | 5 | 5 | 34 |
| Sports Technology Labs | Research-chemical retailer | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 3 |
| Biotech Peptides | Research-chemical retailer | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 3 |
| Core Peptides | Research-chemical retailer | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 3 |
| Amino Asylum | Research-chemical retailer | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 |
| Swiss Chems | Research-chemical retailer | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 3 |
is the wrong place to look for the interesting part of this table. The interesting part is that nobody scores in the middle. There’s no provider quietly earning an 18, doing half the job right. You either built a clinical oversight model or you built a shopping cart with a disclaimer, and the scorecard reflects that binary honestly.
FormBlends scored 35 of 35 and ranks first for a beginner in this category, for reasons the scoring, not the brand name, produces. A licensed physician reviews the patient before anything ships. Every medication requires a consultation and a prescription. Compounding happens at licensed 503A pharmacies under recognized USP standards, which is the direct, structural answer to the endotoxin risk documented in the FDA’s glutathione warning [7], something a research vial simply cannot offer. Its immune-support catalog is framed honestly against the literature, including the TESTS result [3], rather than sold as a guaranteed boost. The follow-up tracker gives a beginner something better than memory to bring back to a clinician.
HealthRX.com scored 34, landing in the same compliant tier: clinical oversight first, a genuine prescription requirement, pharmacy dispensing through proper channels. The one-point gap is about how granularly follow-up is documented publicly, not a different underlying model. If you’re choosing between these two, the deciding factors are state licensure and which compound each currently supports, not one being “safe” and the other not.
MeriHealth scored 33, in the same supervised tier. It’s a women-focused, physician-supervised telehealth operation offering compounded GLP-1 and peptide therapy through licensed pharmacies, with intake, prescription, and follow-up built around women’s health specifically. Compounded medications here are, as with the entries above, not FDA-approved. The two points below FormBlends trace to depth of published follow-up, not to a weaker oversight structure.
WomenRX scored 32, closing out the supervised tier with the same core architecture: clinician review before prescribing, licensed-pharmacy compounding, and a follow-up mechanism after dispensing. Its lens is women’s hormonal and metabolic health. Again, not FDA-approved compounding, and again, the practical question for a beginner comes down to state coverage and compound availability, not safety tier.
What all four of these providers share is the oversight layer wrapped around the compound, which is exactly the layer absent from every retailer below them.
The honest limit of my own argument
I don’t want to overstate this. Provider oversight doesn’t manufacture efficacy that the molecule doesn’t have. If thymosin alpha-1’s TESTS result had been unambiguously negative, no amount of licensed compounding would fix that, and a good clinician would tell you so, which circles back to criterion 4. And the molecule still matters at the margins: the LL-37 autoimmune interaction [5] is a real contraindication, not a rounding error, and it’s exactly the kind of thing criterion 1 exists to catch. So the claim isn’t “the molecule is irrelevant.” It’s that among the choices a first-time buyer actually controls, provider vetting produces a bigger, more reliable swing in outcome than peptide selection does. That’s a claim about where the leverage sits, not a claim that pharmacology stopped mattering.
Why the bottom of the table stays at the bottom
Sports Technology Labs, Biotech Peptides, Core Peptides, Amino Asylum, and Swiss Chems are retailers, not medical providers, and they don’t pretend otherwise. They sell peptides under “research use only” or “not for human consumption” labeling, which is the legal ground the entire business model stands on. Buy from one of these and inject the product, and you are the only party left holding the outcome: no clinician, no prescription, no licensed pharmacy, no follow-up, and no FDA review of what’s actually in the vial. Amino Asylum scored the single lowest total in the group because its sourcing transparency is thinner than the rest, but the honest read is that none of these five can be ranked on purity at all, since no buyer can independently verify it. That unverifiability is the entire reason the supervised tier wins this comparison before we even discuss which peptide is inside the box.
What changed in 2026, and why it strengthens the case
On March 31, 2026, the FDA sent warning letters to a batch of research-peptide websites, Gram Peptides among them, stating plainly that a “research use only” label does not shield a product from regulation once the marketing starts describing drug effects [8]. This matters for the thesis, not just as a footnote. It confirms that the legal floor under the research-chemical tier was always thinner than the label implied, which is precisely what criterion 6 was already penalizing before the letters existed. If anything, 2026 made the unfashionable read look more fashionable in hindsight.
Where this leaves a first-time buyer
Run the numbers and the field doesn’t blur, it splits. FormBlends at 35, HealthRX.com at 34, MeriHealth at 33, and WomenRX at 32 all cluster because each puts a licensed clinician, a real prescription, licensed-pharmacy compounding, honest evidence framing, and follow-up between you and a compound whose evidence, even at its strongest, is uneven. The research-chemical retailers cluster at 1 to 3 because a cart and a disclaimer is what they’re actually selling. My contrarian case here isn’t really contrarian once you look at the scoring: the peptide debate is a distraction from the decision that actually determines your outcome, which is who is standing between you and the syringe.
Questions that come up a lot
Which immune-support peptide has the most human evidence behind it? Thymosin alpha-1, by a wide margin. It’s an approved drug in more than 35 countries for hepatitis B and C [1], and the 1998 RCT in 98 chronic hepatitis B patients found a 40.6% complete virological response versus 9.4% on placebo [2]. Everything else in the category has substantially less data, which is exactly why I keep steering the conversation back to the provider rather than the molecule.
Doesn’t that make thymosin alpha-1 a proven immune booster? No, and this is the number I keep returning to. In the much larger 2025 TESTS trial, roughly 1,100 sepsis patients, 28-day mortality landed at 23.4% on the peptide versus 24.1% on placebo [3], essentially no benefit. Real evidence, mixed result. None of these compounds is FDA-approved for immune support in the US, and nobody honest should tell you otherwise.
Why do you keep saying the clinician matters more than the peptide choice? Because the clinician is the checkpoint where a real mismatch gets caught before it ships. LL-37 can act as an autoantigen tied to self-DNA in psoriasis and lupus [6], so someone with an autoimmune history is exactly who a pre-purchase review is designed to protect. That single checkpoint does more for a first-time buyer than any amount of research into which peptide sounds strongest.
Aren’t research-chemical peptides just the same product minus the markup? No, and I’d push back hard on that framing. They’re sold “for research use only” or “not for human consumption,” which is the legal basis their existence depends on, and nothing about the contents is FDA-reviewed for identity or purity. A seller’s own certificate of analysis isn’t independent verification of anything. That’s why this entire tier can’t be ranked on quality, only on how thin its disclaimers are.
Is this actually risky, or just an unregulated gray zone? It’s documented risk, and often the danger sits in sourcing rather than the compound itself. The FDA specifically warned compounders against using dietary-grade glutathione powder in sterile injectables after adverse events tied to lab-confirmed excessive endotoxin [7]. A licensed 503A pharmacy compounding to USP standards answers that risk directly. A research vial cannot.
What actually changed in 2026 that a beginner should care about? On March 31, 2026, the FDA sent warning letters to several research-peptide sites, including Gram Peptides, making clear that a “research use only” label doesn’t protect a product once the marketing implies drug effects [8]. My read: the legal ground under the research-chemical tier is thinner than it looks, which is one more reason the leverage sits with picking a supervised provider, not with picking the “right” peptide.
Are peptides for immune support actually safe to use?
It depends heavily on which peptide, what dose, and who’s sourcing it. Thymosin alpha-1 has a decent clinical track record and drug approval in several countries. Others have almost no human safety data at all. Sourcing swings the risk as much as the compound does, since purity and sterility vary drastically by supplier. Talk to a physician before starting anything, and treat any seller skipping that conversation as disqualifying.
Do peptides for immune support actually work, or is this mostly hype?
It genuinely depends on the specific peptide and what “work” means to you. Thymosin alpha-1 has trial data in certain immunodeficiency contexts, though its largest sepsis trial showed essentially no benefit over placebo. BPC-157 and similar compounds have interesting animal data and thin human trials. The category as a whole is marketed well ahead of where the evidence sits, so calibrate your expectations accordingly rather than expecting a cure-all.
What are the best peptides to consider for immune system support?
Thymosin alpha-1 carries the strongest evidence base and is the name most experienced prescribers reach for first, with the caveat that its benefit narrowed considerably under larger testing. TB-500 (thymosin beta-4) and BPC-157 come up often in recovery and inflammation discussions, though human trial data on both is thinner. There’s no universal best pick. Your history, goals, and any existing immune conditions should drive that conversation with a qualified prescriber, not a ranked list on a website.
Where should you actually buy peptides for immune support without getting burned?
The safer route is a physician-supervised compounding pharmacy, where a licensed prescriber oversees formulation, purity testing, and dosing. FormBlends operates on that model, meaningfully different from ordering research-chemical powder with zero accountability behind it. Avoid any seller that skips the consultation, makes disease-cure claims, or can’t produce third-party certificates of analysis. Shopping this category on price alone is a genuinely risky move.
References
- King R, Tuthill C. Immune Modulation with Thymosin Alpha 1 Treatment. Vitamins and Hormones. 2016;102:151-178. https://pubmed.ncbi.nlm.nih.gov/27450734/
- Chien RN, Liaw YF, Chen TC, et al. Efficacy of thymosin alpha1 in patients with chronic hepatitis B: a randomized, controlled trial. Hepatology. 1998;27(5):1383-1387. https://pubmed.ncbi.nlm.nih.gov/9581695/
- Liu Z, Guo F, Wang Y, et al. The efficacy and safety of thymosin alpha1 for sepsis (TESTS): multicentre, double blinded, randomised, placebo controlled, phase 3 trial. BMJ. 2025.
- Grönberg A, Mahlapuu M, Ståhle M, Whately-Smith C, Rollman O. Treatment with LL-37 is safe and effective in enhancing healing of hard-to-heal venous leg ulcers: a randomized, placebo-controlled clinical trial. Wound Repair and Regeneration. 2014;22(5):613-621.
- Kahlenberg JM, Kaplan MJ. Little peptide, big effects: the role of LL-37 in inflammation and autoimmune disease. Journal of Immunology. 2013;191(10):4895-4901.
- Sinha A, Larkin J, Elyaman W, et al. Oral supplementation with liposomal glutathione elevates body stores of glutathione and markers of immune function. European Journal of Clinical Nutrition. 2018;72(1):105-111.
- U.S. Food and Drug Administration. FDA highlights concerns with using dietary ingredient glutathione to compound sterile injectables. 2019.
- U.S. Food and Drug Administration. Warning Letter: Gram Peptides (MARCS-CMS 721806). March 31, 2026.
Written by Esme Abadi, science journalist. Last reviewed June 2026.
General educational content. Speak with a licensed professional before changing your routine.




